

How it Works
How to Use
How it Works
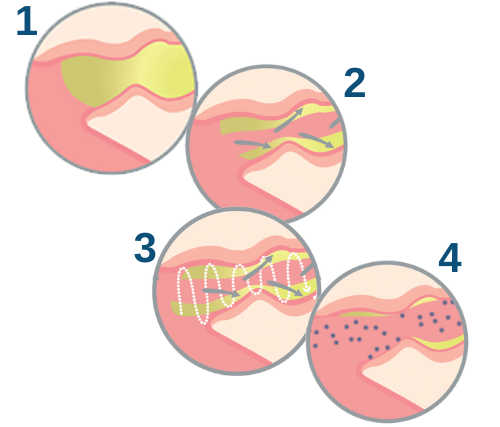
- Before Use: Airways inflamed, collapsed, and plugged with mucus.
- As you exhale through the device, positive pressure will hold the airways open. Think of how you feel when you blow up a balloon. It is the positive pressure that holds the balloon open. Inside your lungs, the positive pressure opens up small airways that may be blocked by mucus.
- As the airways open, the device switches quickly between higher and lower resistance. This may feel like vibrations or pulses which act to loosen the mucus from the walls of your lungs. The frequency of the oscillations closely match the ones within your lungs, helping move mucus to the larger airways. This makes it easier for you to cough up the secretions.
- With the airways opened and the mucus moved out of the airways, your inhaled medication may work better.2
How to Use
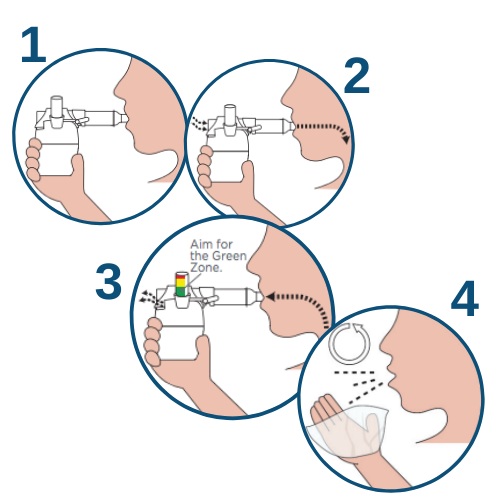
- CLOSE LIPS around mouthpiece
- INHALE and HOLD for 2-3 seconds
- EXHALE – slowly but firmly
- REPEAT as directed
These are shortened user instructions. Always review the complete instructions that came with your device.



